Internal Medicine – Hyponatremia: By Andrew House M.D.
Автор: Medskl.com
Загружено: 2017-09-15
Просмотров: 11052
Описание:
medskl.com is a global, free open access medical education (FOAMEd) project covering the fundamentals of clinical medicine with animations, lectures and concise summaries. medskl.com is working with over 170 award-winning medical school professors to provide content in 200+ clinical presentations for use in the classroom and for physician CME.
Internal Medicine – Hyponatremia
Whiteboard Animation Transcript
with Andrew House, MD
https://medskl.com/module/index/hypon...
Let’s begin with the basics. Measured plasma sodium is a cheap substitute for serum osmolality.
The one golden rule you must remember, is that if the plasma Na+ level is abnormal, it usually means there is a problem with osmolality, and hence with water handling, not Na+ handling.
If the patient has abnormal ECF volume, then there is a problem with Na+ handling.
Hyponatremia is defined as having a plasma Na+ concentration less than 136 mmol/L. In other words, there is too much water relative to Na+. This can result in serious consequences, as it may cause dangerous brain swelling.
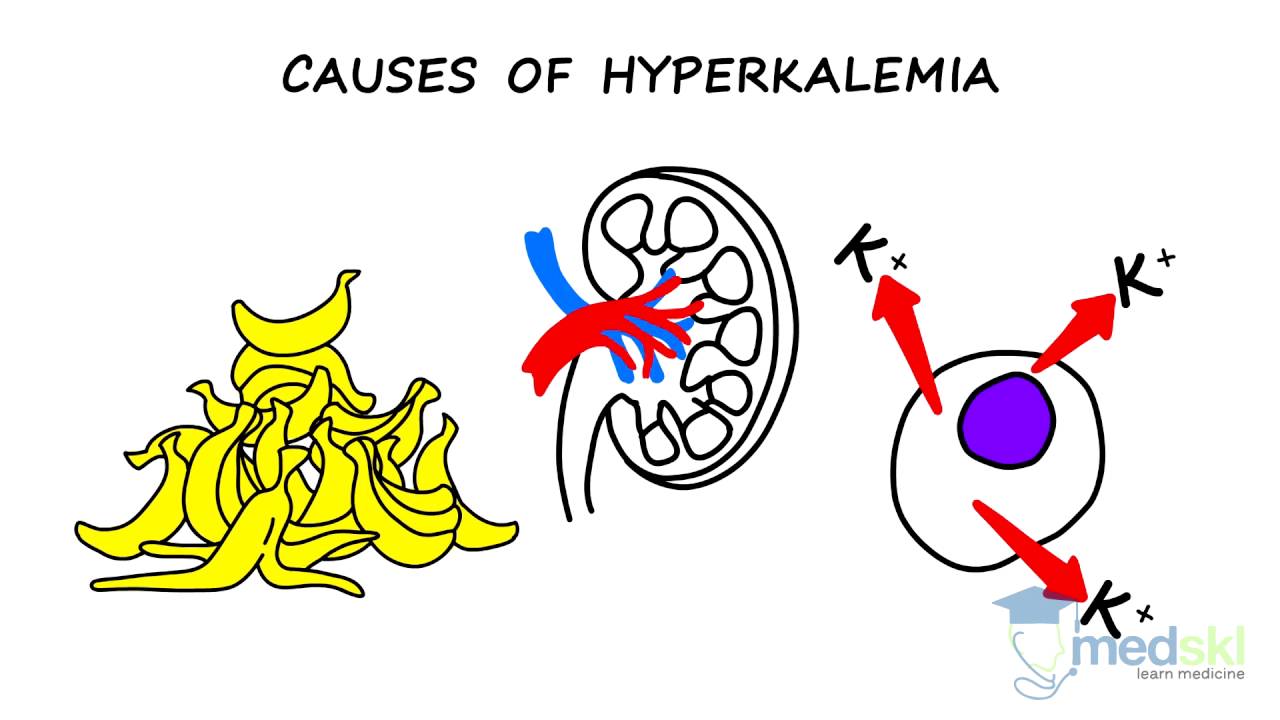
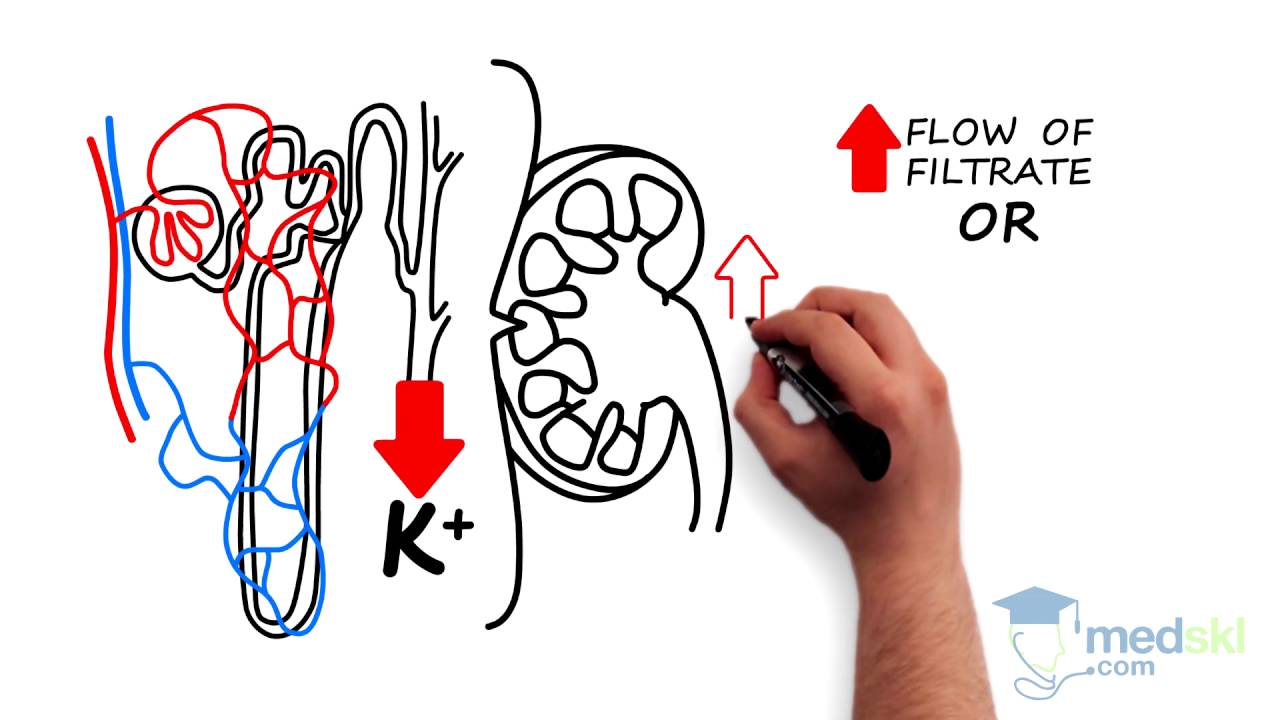
Typically hyponatremia is the result of free water and ADH excess. Normal compensation to low plasma Na+ levels (and low plasma osmolality) should be the excretion of dilute urine. So, you must figure out why the kidneys are not getting rid of the excess water. Important factors to consider include the glomerular filtration rate, renal tubule function, and the etiology of excess ADH release.
When treating patients with hyponatremia, the first step is to identify and correct the underlying cause of excess ADH secretion. It is also imperative for patients to be placed on fluid restriction. However, IV fluids hypertonic to the patient’s urine are indicated in symptomatic patients.
Remember, the regulation of plasma osmolality (as measured by plasma Na+) through the body’s handling of free water is critical in regulating the size of all cells.
If patients are hyponatremic, it can result in dangerous brain swelling. BUT, if you correct for this too quickly, it can cause the problem to shift in the opposite direction – resulting in brain shrinkage and osmotic demyelination.
Therefore, the optimal way to treat hyponatre mic patients is slowly at a rate of less than 8-10 mmol/L per day. The only exception is if patients are symptomatic. In symptomatic patients, treat the first 3-7 mmol/L rapidly, followed by the slower approach.
Повторяем попытку...
Доступные форматы для скачивания:
Скачать видео
-
Информация по загрузке: