Cauda Equina Syndrome (CES)
Автор: EM Note
Загружено: 2025-02-27
Просмотров: 2029
Описание:
Homepage: EMNote.org ■
🚩Membership: https://tinyurl.com/joinemnote
🚩ACLS Lecture: https://tinyurl.com/emnoteacls
Cauda Equina Syndrome (CES)
Case Presentation
Patient Profile:
51-year-old male with acute onset lower back pain after a gym session.
Symptoms: Weakness in lower extremities, pain/numbness in legs (right worse than left).
Pain unrelieved by parenteral diclofenac.
Key Findings on Examination:
Inability to walk on heels.
Distended urinary bladder palpable below umbilicus.
Absence of active/passive anal tone on rectal exam.
Diagnosis
Primary Diagnosis: Cauda Equina Syndrome (CES).
Common Cause: Herniated intervertebral disc (most often at L4/5 level).
Clinical Features:
Lower extremity weakness and pain.
Urinary retention or bowel incontinence.
Loss of anal tone and saddle anesthesia.
Pathophysiology:
Compression of cauda equina nerve roots (S2–4) affecting bladder, sphincters, and perineal sensation.
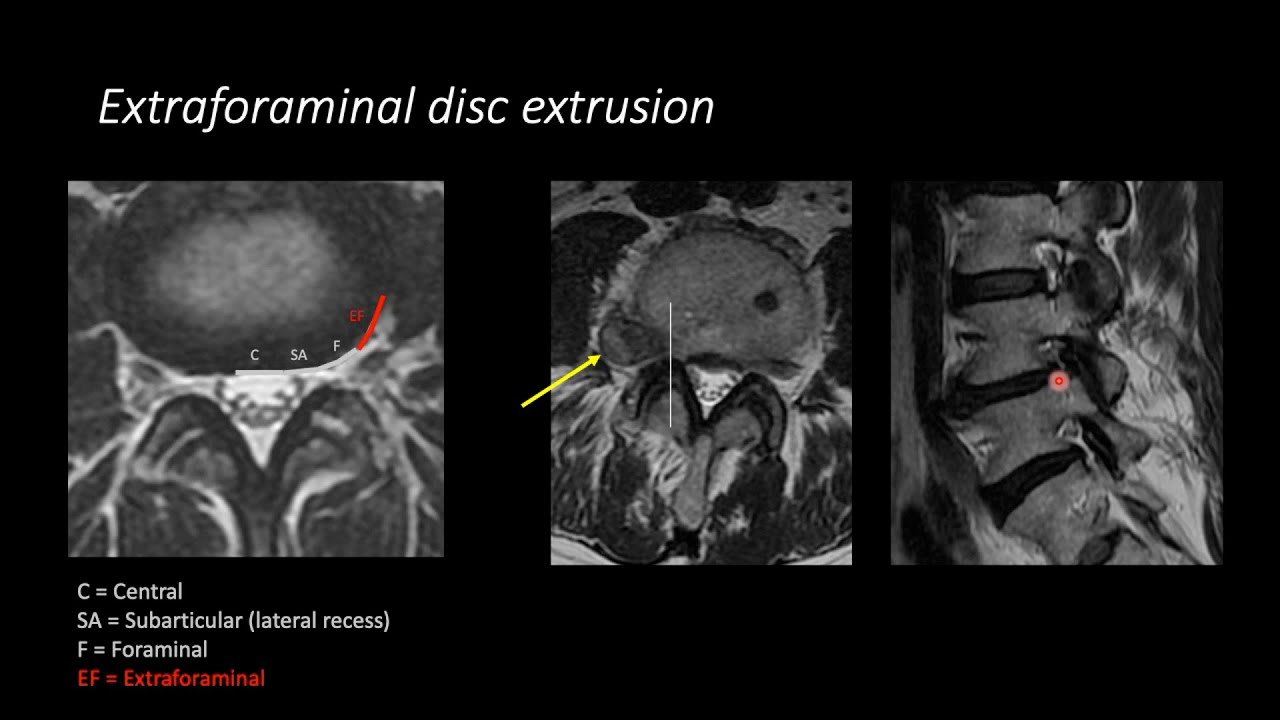
Imaging Studies
Preferred Imaging: MRI of the lumbar spine.
Identifies compression of cauda equina and loss of CSF signal around nerve roots.
Sagittal and axial T2-weighted images are critical.
Alternative Imaging:
Non-contrast CT scan if trauma or bony fractures are suspected.
Faster scan time (seconds to minutes) compared to MRI (30–60 minutes).
Extended Imaging Considerations:
Include thoracic/cervical spine and brain if clinical findings suggest higher-level lesions.
Differential Diagnosis
Conditions Mimicking CES:
Stroke.
Vascular claudication.
Deep venous thrombosis (DVT).
Muscle cramps.
Peripheral neuropathy.
Key Differentiator: Detailed history and physical examination.
Management
Immediate Actions:
Recognize CES as a neurosurgical emergency.
Perform rectal exam to assess anal tone and saddle anesthesia.
Confirm urinary retention using post-void bladder scan.
Timing of Symptoms:
Foot drop developing over 24 hours responds better to urgent decompression.
Chronic symptoms (e.g., weeks of bowel incontinence) may still require surgery to prevent further deterioration.
Preoperative Workup:
Full blood count, electrolytes, coagulation studies, and blood grouping/crossmatching.
Key Takeaways
History and Examination:
A thorough history and rectal exam are essential for diagnosing CES.
Imaging:
MRI is the gold standard; extend imaging if needed to rule out higher lesions.
Timing Matters:
Early surgical intervention improves outcomes, especially for acute symptoms (within 24 hours).
Laboratory Tests:
Obtain preoperative labs early to address abnormalities promptly.
Conclusion
Summary:
CES is a rare but serious condition requiring prompt recognition and intervention.
Maintain a high index of suspicion for CES in patients with lower back pain, weakness, and urinary/bowel dysfunction.
Call to Action:
Prioritize timely diagnosis and surgical referral to prevent irreversible neurological deficits.
Повторяем попытку...

Доступные форматы для скачивания:
Скачать видео
-
Информация по загрузке: