Module 27.3 - Antihypertensive Toxicology - Lecture
Автор: Craig Cocchio
Загружено: 2026-02-01
Просмотров: 6
Описание:
Welcome to Nexus Clinical!
Before diving into this lecture, I want to ensure we're all on the same page.
This is for general informational purposes only and does not constitute the practice of medicine, nursing, or other professional healthcare services, including the giving of medical advice. No doctor-patient or pharmacist-patient relationship is formed. Using this information and the materials linked to this content is at the user's risk. This is not intended to substitute for professional medical advice, diagnosis, or treatment. Users should not disregard or delay seeking medical advice for any medical condition they have, and they should consult their healthcare professionals for any such conditions.
Clinical experts created the references, content, and clinical insight. NotebookLM, a Google AI tool, created the content, which I extensively reviewed before release.
Finally, the host states that he takes all conflicts of interest seriously. Currently, there are no conflicts to disclose. For all of his disclosures and the companies he invests in or advises, he directs users to reach out independently, where he keeps an up-to-date and active list of all disclosures.
Welcome to this critical educational module on Antihypertensive Toxicology, designed to cultivate a profound understanding of these essential medications and their associated toxicologic considerations.
We begin by exploring the historical evolution of pharmacotherapy for hypertension, from first-generation agents developed in the 1960s—including centrally acting sympatholytics, direct vasodilators, and diuretics—to newer classes like ACEIs, ARBs, and DRIs.
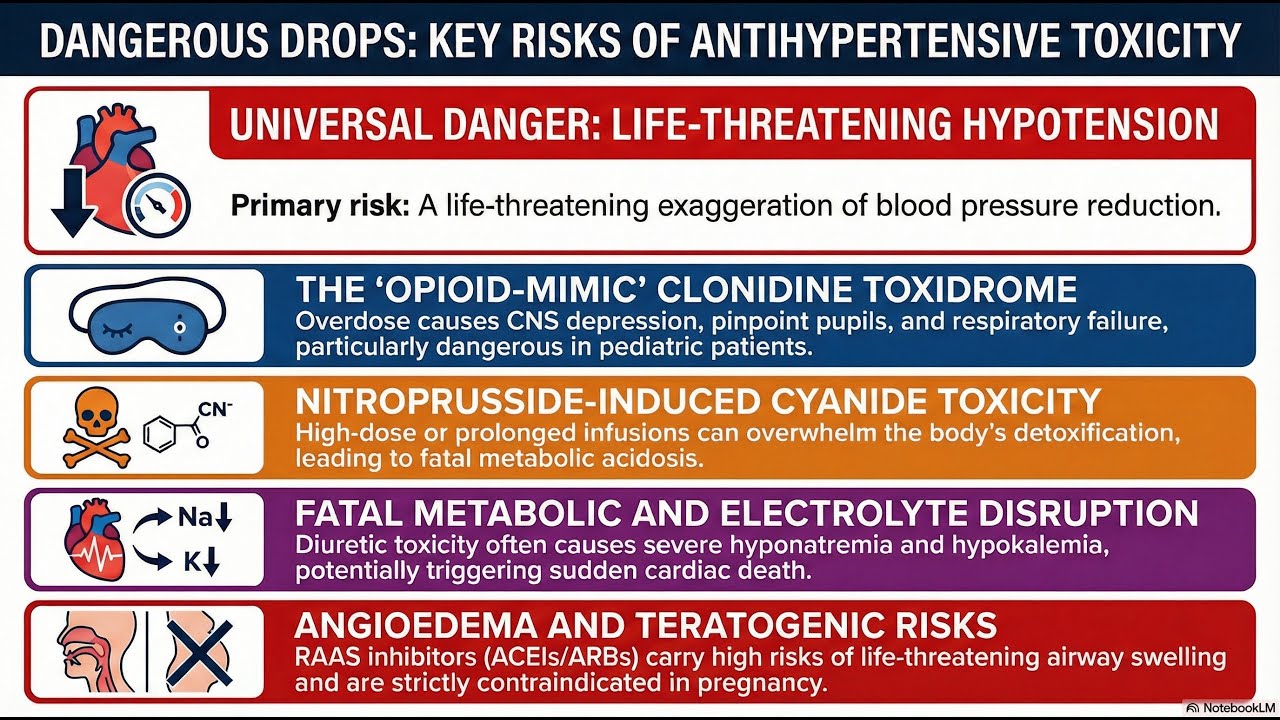
The general principle of toxicity dictates that most antihypertensive overdoses manifest as an exaggeration of pharmacological effects, primarily driven by the degree of hypotension produced.
However, specialized management is required for certain classes:
Centrally Acting Sympatholytics (e.g., Clonidine): Overdose creates a distinct toxidrome mimicking opioid poisoning, characterized by CNS depression, bradycardia, hypotension, and miosis. Management focuses on supportive care, with an empirical trial of high-dose naloxone considered reasonable for refractory respiratory depression. We also emphasize that beta-adrenergic antagonists are contraindicated in clonidine withdrawal due to the risk of paradoxical hypertension.
Direct Vasodilators: We analyze agents like sodium nitroprusside, focusing on the critical risk of cyanide and thiocyanate toxicity, managed with hydroxycobalamin or sodium thiosulfate prophylaxis.
Diuretics: Toxicity is predominantly metabolic, presenting as electrolyte abnormalities (e.g., hyponatremia, hypokalemia) and risks like osmotic demyelination syndrome or ventricular dysrhythmias. Acute overdose management is supportive, focusing on correcting fluid and electrolyte status.
RAAS Inhibitors (ACEIs/ARBs/DRIs): Key adverse events include angioedema and teratogenicity. Overdose typically causes hypotension. For refractory hypotension, novel therapies such as methylene blue or vasopressin may be utilized. Combination therapy with multiple RAAS-acting agents is associated with increased risks, including acute kidney injury and stroke.
This module provides the necessary clinical insights to manage the diverse and unique toxicologic presentations of antihypertensive agents.
Повторяем попытку...
Доступные форматы для скачивания:
Скачать видео
-
Информация по загрузке: